
project draft
Simulation and Reduction of Coercive Measures in Psychiatry (SRZP)
a model project in conflict, violence and prevention research
Project manager: PD Dr. Stephan Debus, Hannover Medical School, Clinic for Psychiatry, Social Psychiatry and Psychotherapy
Mail: info@srzp.de Facebook: www.facebook.com/srzpde Twitter: www.twitter.com/srzpde
Would you want to be a project-FAN on science platform: HERE
1. The problem of “force and coercion” in psychiatry
Despite the initial success of psychiatric reform, more than 100,000 people are still subjected to physical coercion measures in Germany’s psychiatric hospitals and clinics each year. These measures mainly involve forcible restraint, forcible medication and isolation. And psychiatry is just one example: the right to freedom is also forcibly restricted in other areas of medicine and in social fields. It is not only patients who are at increased risk of physical or mental injury as a result but also nurses, who usually carry out these coercive measures. Some groups are at particular risk: they include women who are at greater risk of being traumatised and people from other cultural backgrounds who do not understand German and are therefore less likely to cope with the cultural obstacles encountered in hospital.

Yes – communication fails more often than we think. I should therefore like to introduce to you our research project “Simulation and reduction of coercive measures in psychiatry (SRZP) – a model project in conflict, violence and prevention research”, which is addressing the problem I have just described. We are investigating how force and coercion can be reduced through changed communication and relationship work between nurses and patients within the setting of the psychiatric ward. In our research project we therefore draw on the experience of nurses and patients in order to identify typical communication and relationship patterns in dangerous situations. From this analysis we can then develop alternatives to coercion. Following a two-year pilot phase in which we have worked with three teams from the acute psychiatric wards of two hospitals in the Hannover region and with Hannover Medical School, we now want to launch a comprehensive scientific study that will produce transferrable and verifiable results. Our intention is that the communication analysis and the resulting films will be incorporated into the training of medical practitioners and nurses. On the project website and in social media you can share and recommend the project or take part in the discussion.
2. Methodology: From videos to interaction analysis
Psychodrama has proved very useful for re-enacting direct face-to-face communication and interaction between nurses and patients in dangerous situations. Everyday life on the ward is not filmed directly, since this is prohibited for reasons of confidentiality and medical ethics. And in any case we want to explore things that are not visible, such as the way the people involved interpret the situation, the relationship patterns between them, the behaviour options available and the rules behind the relationship patterns. We are not particularly interested in whether patients are actually dangerous; we are interested in whether patients – in any sort of situation – are regarded as dangerous. Psychodrama works with the change of perspective arising from the different roles that the participants assume. This enables conflicts and “tipping points” (transitions from non-violent to violent situations) to be experienced authentically and at first hand. Typical relationship patterns and differing interpretations of the situation emerge clearly in the re-enactments. This alone enables the participants to reflect on their everyday situation and to learn and try out new ways of communicating
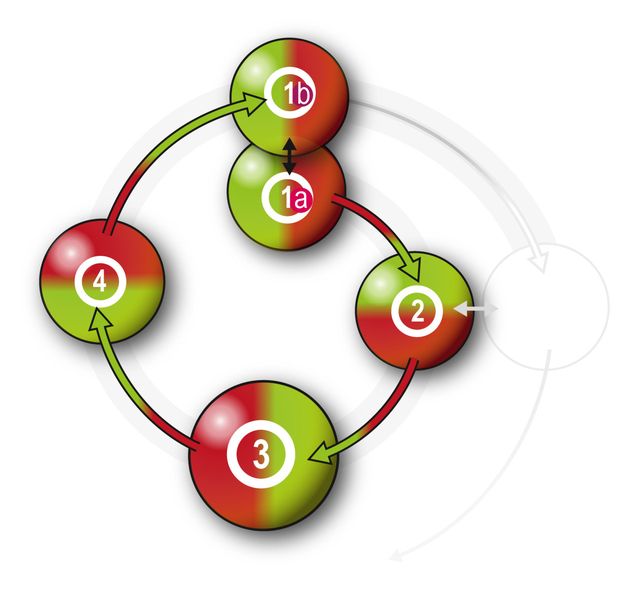
Up to this point the project could be viewed as a type of team training. But we want to conduct fundamental research, because we need transferable, comparable and reproducible results for therapy research. The work program (see Figure 2) has the following cyclical structure: ordinary psychiatric events on an acute ward (1a) are re-enacted through psychodrama (2); they are recorded on video and the film is then analysed. All verbal utterances are transcribed. All non-verbal communications (e.g. gestures, facial expressions, body language) and paraverbal ones (e.g. verbal emphasis, intonation, inflection, the pitch of the voice) are also captured by the annotation system. This enables us to analyse, record and reconstruct on a second-by-second basis the sequence of the communication process and the relationship patterns that arise (3). Details of our methods can be found HERE.
The films and the results of the film analysis are presented to the participants, who review them critically. This provides the basis for expert group interviews (3). We specifically ask the participants about the rules behind the patterns – what rules exist on the ward and what do not; what rules would be desirable and what would not. It is at this stage that the complex rules of dangerous situations emerge, and these rules explain the communication patterns that have been found. This enables each dangerous situation to be reliably classified using criteria that we derive from the communication patterns and the rules. This review and reflection is kept clear and comprehensible in practice through appropriate forms of presentation and skilled facilitation, and it remains linked to experiential knowledge. In addition, the classification means that later we can compare typical dangerous situations across many different hospitals. Through our fundamental research we are providing therapy research with a systematic way of understanding the communication-based development dynamics of force and coercion.
For those who would like an idea of the scope of the SRZP project – partly in order to understand the financing – we use Stage 3 as an example and estimate here the number of communication acts to be analysed: in each cycle of a study unit (SU), about 14 typical routine treatment scenes will be analysed – in all about 56 scenes in four SUs. We know from our pilot project that the analysis involves a lot of work: each scene lasts about 5 minutes and about 30 communication acts occur each minute. That means that the number of acts to be investigated is about 30 [acts/min] * 5 [min] * 14 [scenes] * 4 [SU] = 8400. If there are communication patterns in the routine processes, we shall find them in our data material. And we shall have the opportunity to precisely identify “starting points” for alternative scenarios in dangerous situations.
3. Simulation and alternative scenarios
The results (of Stage 3) provide us with an empirically based categorisation of dangerous situations and typical processes for the routinely applied application of force. With the teams we scan these chronological processes and try to identify “starting points” that could bring about a change in the violent situation (Stage 4). We look for alternative action strategies that prevent situations from “tipping over” and that help replace the physical application of force with symbolic forms of communication. These alternatives are in turn simulated in psychodramatic scenarios, thus enabling their practical feasibility to be tested on the basis of present experience and past learning. In the final stage (1b), initial experiences with the new processes on the ward are collated and documented. This signals the start of a new study cycle.
4. Funding
The project needs funds of EUR 480,298 for staff costs and EUR 192,192 for equipment and materials – EUR 672,490 in all. For start-up funding and to publish our research videos we need EUR 20,000 initially. Each additional EUR 20,000 will be used for grants to doctoral students and to fund further study units. You can find further details HERE.
5. Prospects and practical impacts
To enable the results to have an impact beyond the project itself, it is important that they are fed into a public debate. In particular, we regard “trialogue” conferences, such as those of the German Society for Social Psychiatry, as a promising way forward. Such conferences provide an opportunity to pursue “trialogue” – that is, communication between users of psychiatric services, family members and professionals – in some depth. We shall participate in the trialogue with information about our research project. Through the methods and results of the research project we promote mutual understanding between participants and put the ideologically inflamed discussion on a more objective footing. Simply addressing this issue gives both patients and nurses a greater feeling that their commitment to safer and freer psychiatry is valued. The videos and accompanying situational analyses produced in the research project contribute to training in the health professions (nursing, social work, medicine, care science, public health, etc.) and can thus be passed on in easily assimilated form.
5.1. Impacts on staff
In the pilot phase we have been able to work with nurses to try out new therapeutic techniques – such as the use of an “auxiliary ego” – as part of our work program. How these techniques work in the eyes of a team, what opportunities and risks they entail and what requirements patients, staff and situations must meet if new strategies are to work successfully – we call these shared and implicit beliefs an “ethnotheory”. Our research project will bring many new ethnotheories to light. Reflection on these implicit beliefs ultimately enables the creative potential of staff to develop more effectively and be used with greater confidence.
5.2. Impacts on patients
Patients very often experience the use of force as a crossing of boundaries; it may even traumatise them anew. The project identifies ways of dealing with such “boundary violations” by establishing contact between the different subjective points of view through a change of perspective, thereby enabling communication to take place. The SRZP project identifies rules and conditions that contribute to success. Because patients are involved in the methodology of the research project, they are not research subjects but “contemporary eyewitnesses” who, like the nurses, make their knowledge available.p>
5.3. Impacts on the psychiatric system
Since psychiatry adapts so that it makes greater use of the extensive knowledge and experience of both staff and patients, the hospital becomes an innovation centre for the prevention of violence. And more: psychiatry uses its expertise to put forward methods that can also be used to reduce force and coercion in somatic medicine (emergency medicine, intensive care, internal medicine, etc.). At this point we should also like to mention the expert interviews that were conducted to complement this project outline and that can likewise be viewed at www.srzp.de. The project results will also have a potential impact in other social fields, such as the emergence of violence in branches of government agencies, in the transport system or at football matches.
5.4. Impacts on the ward environment
Many of the results of the research project relate to the design of the psychiatric ward environment. This refers both to the setting for relationship work and to the architecture and ward atmosphere. The use of coercion tends to make the atmosphere on the ward tense; for everyone involved it does little to inspire confidence. The research literature contains a great deal of evidence that even small changes in the ward environment can have major impacts in terms of enabling a supportive therapeutic atmosphere to develop. Our research project improves our understanding of how the design of the environment changes communication in dangerous situations.
5.5. Impacts on psychiatric and nursing training
The experience and knowledge of those involved in psychiatry and nursing highlights alternative courses of action. The SRZP project promotes reflection on and development of the understanding of professional roles that is acquired during training. If this knowledge is also incorporated into training courses in other fields (e.g. social work,training of judges, patient complaint services, training of non-professionals), synergies with colleagues in other professional groups can be expected too..
5.6. Impacts on psychiatric research
Wenn psychiatrische Milieus und die in ihnen auftretenden Gefahrensituation in ihrer Typik besser verstanden sind, dann hat dies auch Rückwirkung auf die psychiatrische Therapieforschung mit ihrer Suche nach Prädiktoren und Wirkfaktoren.
Gefahrensituationen können anhand bestimmter Anzeichen eindeutiger identifiziert werden. Und dies erlaubt die Untersuchung der Wirksamkeit von therapeutischen Interventionen in vergleichbaren Situationen, d.h. unter gleichen Bedingungen, was eine zentrale Voraussetzung für sog. Interventionsstudien ist.
Better understanding of typical psychiatric settings and the dangerous situations that occur in them also has an impact on psychiatric therapy research and its search for predictors and effect factors. Dangerous situations can be clearly identified from certain signs. And this enables the effectiveness of therapeutic interventions to be investigated in comparable situations – i.e. under the same conditions, which is a key requirement of intervention studies. The use of methods taken from cultural studies enriches psychiatric research. For example, a communication theory (semiotics) is needed that incorporates verbal, preverbal and non-verbal communications from the point of view of the use of signs for the film analysis. Our research method has many similarities with language research, which explores the grammar of a language with the help of competent speakers. More on this HERE.
6. Summary
If the SRZP research project helps to reduce the extent of force and coercion in psychiatry, this will have positive impacts on the quality of life, quality of treatment and quality of work of everyone involved.
It is about deliberate handling of the demands and opportunities of a situation in order to make competent, appropriate and integrative decisions that result in more self-determination and respect for human rights – without losing sight of the fact that there can be situations in which it is necessary to restrict personal freedom. The aim is to find new states of equilibrium between mutually exclusive requirements and to provide clear justification for them.
To achieve this we need a scientifically based debate at the level of comparable results. This will also help to make the discussion more objective. Such debate provides the momentum for progressive psychiatric reform that moves away from increasing automation, video surveillance, prescription of medication, use of robots, routine treatment and bureaucracy and instead advocates mutual understanding, more communication and more relationship work in psychiatric hospitals..
There are choices to be made with regard to the strategic direction of psychiatry. Help to decide what sort of psychiatry you want to support and what sort of world you would like yourself and others to live in.